กลุ่มอาการก่อนมีประจำเดือน
Premenstrual syndrome
นพ. หาญณรงศ์ ชูพูล
อาจารย์ที่ปรึกษา รศ.พญ. ทวิวัน พันธศรี
ประจำเดือนเป็นสิ่งที่เกิดขึ้นกับผู้หญิงทุกคนเมื่อเริ่มเข้าสู่วัยเจริญพันธุ์ การมีประจำเดือนเกิดภายใต้อิทธิพลของการเปลี่ยนแปลงฮอร์โมนเพศในร่างกาย ซึ่งก่อนช่วงที่ผู้หญิงจะมีประจำเดือน บางรายอาจมีอาการที่แสดงออกทั้งทางกาย พฤติกรรม อารมณ์และจิตใจ นั่นคือกลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) ซึ่งอาการเหล่านี้สามารถส่งผลกระทบที่รุนแรงต่อการใช้ชีวิตประจำวันได้ แต่อาการเหล่านั้นจะดีขึ้นหรือหมดไปภายหลังประจำเดือนมา
คำจำกัดความ (Definition)1
กลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) หมายถึงกลุ่มอาการที่ส่งผลต่อร่างกาย พฤติกรรม อารมณ์และจิตใจ ที่เกิดขึ้นในช่วงก่อนมีประจำเดือนของรอบเดือนนั้น และอาการจะหายไปได้เองในช่วงที่มีประจำเดือน
สาเหตุและความชุกของโรค (Etiology and Prevalence)1-3
ปัจจุบันยังไม่ทราบสาเหตุที่แน่ชัดที่ทำให้เกิดกลุ่มอาการก่อนมีประจำเดือน แต่จากการศึกษาพบว่า เกิดจากการเปลี่ยนแปลงของระดับฮอร์โมนแอสโตรเจนและโพรเจสเตอโรน (estrogen and progesterone) ที่มีการเปลี่ยนแปลงในแต่ละช่วงของรอบเดือน ไปกระตุ้นทำให้เกิดอาการก่อนมีประจำเดือนได้ อย่างไรก็ตาม ระดับฮอร์โมนเพศ ก็ไม่สามารถอธิบายสาเหตุการเกิดอาการก่อนมีประจำเดือนได้ทั้งหมด เนื่องจากจากการศึกษา ในผู้หญิงที่ถูกวินิจฉัยว่าเป็นกลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) ก็มีระดับฮอร์โมนเพศที่ปกติได้4 นอกจากนั้น สาเหตุอื่นๆ ได้แก่ การเปลี่ยนแปลงที่มีผลต่อสารสื่อประสาท เช่น Serotonin หรือ gamma-aminobutyric acid (GABA) system ซึ่งจากการศึกษาพบว่า ผู้ป่วยที่มีกลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) จะมีระดับ serotonin ในเลือดลดลง4 และการเพิ่มขึ้นของระดับ Aldosterone และ plasma renin เป็นต้น
ผู้หญิงมากกว่า 80 เปอร์เซ็นต์ สามารถพบกลุ่มอาการที่ส่งผลต่อร่างกาย พฤติกรรม อารมณ์และจิตใจ ในในช่วงก่อนมีประจำเดือน และ 20-32 เปอร์เซ็นต์ของกลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) มักมีอาการในระดับน้อยถึงปานกลาง (mild to moderate symptoms) และพบอาการระดับรุนแรงประมาณ 3-8 เปอร์เซ็นต์ โดยความชุกของกลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) ไม่ได้สัมพันธ์กับอายุ การศึกษา รายได้ และการทำงาน
อาการทางคลินิก ( Clinical manifestation) 2, 5
กลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) แบ่งอาการแสดงเป็น 2 กลุ่ม ได้แก่ อาการทางร่างกาย (Physical symptoms) และอาการทางพฤติกรรม อารมณ์และจิตใจ (Behavioral and psychological symptoms)
- อาการทางร่างกาย (Physical symptoms) ได้แก่ ท้องอืด (Abdominal bloating) คันตามร่างกาย (Body aches) เจ็บบริเวณเต้านม (Breast tenderness) เกร็งท้อง ปวดท้องมากขึ้น (Cramps/ Abdominal pain) เพลีย (Fatigue) ปวดศีรษะ (Headaches) คลื่นไส้ (Nausea) แขนขาบวม (Swelling of extremities) น้ำหนักขึ้น(Weight gain) เป็นต้น
- อาการทางพฤติกรรม อารมณ์และจิตใจ (Behavioral and psychological symptoms) ได้แก่ โกรธง่าย หงุดหงิด (Anger, irritability) กังวล (Anxiety) ความอยากอาหารเปลี่ยน (Changes in appetite) ความสนใจทางเพศเปลี่ยนไป (Changes in libido) ไม่มีสมาธิ (Decreased concentration) ซึมเศร้า (Depressed mood) อารมณ์แปรปรวนง่าย (Mood swings) นอนไม่หลับ (Poor sleep or increase need for sleep) เครียด (Tension) เป็นต้น
การวินิจฉัย (Diagnosis) 1, 2, 5
การวินิจฉัยกลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) ตามแนะนำ ACOG ขึ้นกับการติดตามจดบันทึกอาการต่างๆที่เกิดขึ้น โดยใช้ “Daily Record of Severity of Problems (DRSP)” ดังตารางแสดงที่ 2 ซึ่งมีค่า Positive predictive value เท่ากับ 53.8 เปอร์เซ็นต์ และ Negative predictive value เท่ากับ 83.4 เปอร์เซ็นต์ โดยการบันทึกจะเป็นการบันทึกแบบไปข้างหน้า (Prospective) ติดต่อกันอย่างน้อย 2 รอบเดือน และต้องแยกกลุ่มอาการที่เกิดจากสาเหตุอื่นๆออก เช่น ภาวะไทรอยด์ต่ำ (Hypothyroidism) ภาวะซีด (Anemia) ภาวะเยื่อบุโพรงมดลูกเจริญผิดที่ (Endometriosis) เป็นต้น
นอกจากนั้นตามคำแนะนำ ACOG (2014) แนะนำการวินิจฉัยกลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) ผู้ป่วยจะต้องมีอย่างน้อย 1 อาการจากอาการทางร่างกาย และอย่างน้อย 1 อาการจากอาการทางจิตใจ ดังแสดงในตารางที่ 1 ที่แสดงอาการภายใน 5 วันก่อนประจำเดือน อย่างน้อย 3 รอบเดือนติดต่อกัน และอาการจะต้องหายไปภายใน 4 วัน หลังจากเริ่มมีประจำเดือน และอาการที่แสดงจะต้องส่งผลกระทบต่อชีวิตประจำวัน
| Affective symptoms | Somatic symptoms |
| Angry outbursts | Abdominal bloating |
| Anxiety | Breast tenderness or swelling |
| Confusion | Headache |
| Depression | Joint or muscle pain |
| Irritability | Swelling of extremities |
| Social withdrawal | Weight gain |
ตารางที่ 1 Diagnostic criteria for premenstrual syndrome 1
นอกจากนั้น หากผู้ป่วยมีอาการ premenstrual syndrome ชนิดรุนแรง อาจวินิจฉัยเป็น Premenstrual dysphoric disorder (PMDD) เกณฑ์การวินิจฉัยตาม Diagnostic and Statistical Mental disorder fifth edition (DSM-V) ของ American Psychiatric Association 1
A. In the majority of menstrual cycles, at least five symptoms must be present in the final week before the onset of menses, start to improve within a few days after the onset of menses, and become minimal or absent in the week postmenses.
B. One (or more) of the following symptoms must be present:
- Marked affective lability (e.g., mood swings; feeling suddenly sad or tearful, or increased sensitivity to rejection).
- Marked irritability or anger or increased interpersonal conflicts.
- Marked depressed mood, feelings of hopelessness, or self-deprecating thoughts.
- Marked anxiety, tension, and/or feelings of being keyed up or on edge.
C. One (or more) of the following symptoms must additionally be present, to reach a total of five symptoms when combined with symptoms from Criterion B above.
- Decreased interest in usual activities (e.g., work, school, friends, hobbies).
- Subjective difficulty in concentration.
- Lethargy, easy fatigability, or marked lack of energy.
- Marked change in appetite; overeating; or specific food cravings.
- Hypersomnia or insomnia.
- A sense of being overwhelmed or out of control.
- Physical symptoms such as breast tenderness or swelling, joint or muscle pain, a sensation of “bloating,” or weight gain.
NOTE: The symptoms in Criteria A–C must have been met for most menstrual cycles that occurred in the preceding year.
D. The symptoms are associated with clinically significant distress or interference with work, school, usual social activities, or relationships with others (e.g., avoidance of social activities; decreased productivity and efficiency at work, school, or home).
E. The disturbance is not merely an exacerbation of the symptoms of another disorder, such as major depressive disorder, panic disorder, persistent depressive disorder (dysthymia), or a personality disorder (although it may co-occur with any of these disorders).
F. Criterion A should be confirmed by prospective daily ratings during at least two symptomatic cycles. (NOTE: The diagnosis may be made provisionally before this confirmation.)
G. The symptoms are not attributable to the physiologic effects of a substance (e.g., a drug of abuse, a medication, other treatment) or another medical condition (e.g., hyperthyroidism).
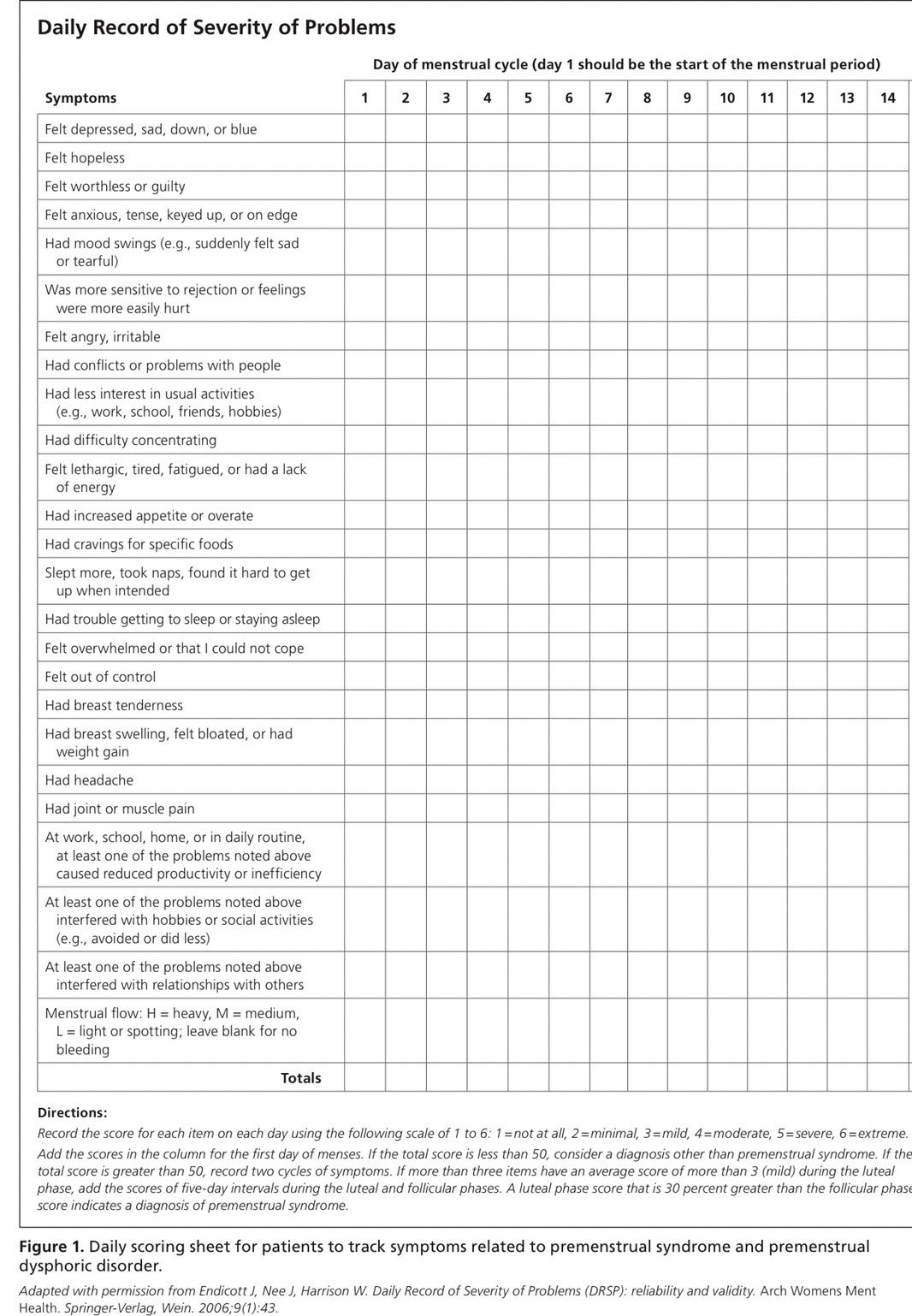 ตารางที่ 2 Daily Record of Severity of Problems (DRSP) 2
ตารางที่ 2 Daily Record of Severity of Problems (DRSP) 2
การรักษา (Treatment) 1-3, 6-11
การรักษากลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) มุ่งเน้นเพื่อลดอาการทางร่างกาย อารมณ์ และจิตใจที่มีการเปลี่ยนแปลงไป ในการรักษาแบ่งออกเป็น 3 ประเภท ได้แก่
1. การรักษาแบบที่ไม่ใช้ยา (Non-Pharmacologic treatment)
1.1 การปรับเปลี่ยนพฤติกรรม (life style modification) เช่น การออกกำลังกาย หลีกเลี่ยงการรับประทานอาหารที่มีน้ำตาล โซเดียม และคาเฟอีนที่มีประมาณมาก เป็นต้น
1.2 การรัปประทานแคลเซียมและวิตามินดี (Dietary Calcium and vitamin D intake) ผู้หญิงที่มีอาการก่อนมีประจำเดือน (Premenstrual syndrome) ในด้านอารมณ์ที่เปลี่ยนแปลง (Mood instability) มีความสัมพันธ์กับระดับแคลเซียมในร่างกาย แต่ไม่ทราบกลไกที่แน่ชัด การศึกษา RCT จาก Tehran university1 พบว่า นักศึกษาที่ได้รับการวินิจฉัย Premenstrual syndrome จำนวน 179 คน พบว่า นักศึกษาที่ได้รับประทาน Calcium carbonate 1000 mg เป็นระยะเวลา 3 เดือน มีอาการซึมเศร้า เพลีย ลดลงถึง 50 เปอร์เซ็นต์ อีกการศึกษาหนึ่ง 7 พบว่า ผู้หญิงที่รับประทาน calcium carbonate 1200 mg ต่อวันเทียบกับ placebo ในระยะเวลา 3 เดือน พบว่า มีการลดลงทั้ง Somatic symptoms และ affective symptoms 48 เปอร์เซ็นต์
การรับประทานวิตามินดี (Vitamin D supplementation) ในการรักษา Premenstrual syndrome จากการศึกษา cross-sectional analysis of a large study พบว่า ระดับวิตามินดีที่ต่ำลง ไม่ได้สัมพันธ์กับการเกิดอาการก่อนมีประจำเดือน (Premenstrual syndrome) ที่เพิ่มมากขึ้น
1.3 จิตบำบัด (Cognitive Behavior Therapy) เป็นการทำจิตบำบัดชนิดหนึ่งที่มีการใช้เทคนิค Psychotherapy เพื่อปรับเปลี่ยนความคิด อารมณ์ และพฤติกรรมของผู้ป่วยรายนั้น จากการศึกษา Meta-analysis 2009 (7 trial) 1 พบว่า การใช้ Cognitive Behavior Therapy ในการรักษา Premenstrual syndrome มีระดับคะแนนการทำงานและอาการซึมเศร้าที่ดีขึ้น แต่ยังไม่ทราบแน่ชัดในเรื่องของความถี่และระยะเวลาในการรักษา
1.4 แพทย์ทางเลือก (Complementary and alternative therapies) จากการศึกษา Cochrane review 2010 1 พบว่า การใช้สมุนไพรจีนในการักษากลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) ยังไม่พบหลักฐานที่แน่ชัด นอกจากนั้น การศึกษา Systemic review 2009 (62 studies) 2 พบว่า การใช้ Gingko, Saffron, St. John’s wort, Soy และ vitamin E ยังไม่มีข้อมูลที่เพียงพอในการรักษา แต่พบว่า Chasteberry (Vitex agnus-castus) และ Vitamin B6 สามารถช่วยลดอาการก่อนมีประจำเดือน (Premenstrual syndrome) ได้ โดย Vitex agnus-castus ยังไม่ทราบกลไกที่แน่ชัด แต่การศึกษา in vitro พบว่า Vitex agnus-castus ไปจับกับ Dopamine-2 receptor และ Opioid receptor และไปมีผลต่อ estrogen receptor และ Vitamin B6 มีผลทำให้มีการเพิ่มขึ้นของระดับ Serotonin Norepinephrine Histamine Dopamine และ Taurine ที่ช่วยลดอาการ Premenstrual syndrome 7 โดยแนะนำให้ใช้ vitamin B6 80 mg ต่อวัน
2. การรักษาแบบที่ใช้ยา (Pharmacologic treatment)
2.1 Serotonergic antidepressants ถือเป็นยาทางเลือกหลักในการรักษา Premenstrual syndrome (first line drugs) ยาในกลุ่มนี้ประกอบไปด้วย SSRIs (selective serotonin reuptake inhibitors) เช่น Sertraline (Zoloft) Paroxetine (Paxil) Fluoxetine (Prozac) Citalopram (Celexa) Escitalopram (Lexapro) เป็นต้น และ SNRIs (serotonin – norepinephrine reuptake inhibitors) เช่น Venlafaxine (Effexor) เป็นต้น จากการศึกษา Cochrane review 2013 1 พบว่า การใช้ SSRIs เทียบกับ placebo มีการลดลงของอาการของ Premenstrual syndrome อย่างมีนัยสำคัญทางสถิติ นอกจากนั้นมีการสนับสนุนว่า การใช้ SNRIs (serotonin – norepinephrine reuptake inhibitors) ในการรักษาผู้ป่วย PMDD ด้วย ผลข้างเคียงที่เกิดขึ้นจากการใช้ยาในกลุ่มนี้ เช่น คลื่นไส้อาเจียน เพลีย นอนไม่หลับ ปวดศีรษะ และความรู้สึกทางเพศเปลี่ยนไป เป็นต้น
2.2 Oral contraceptives ถูกนำมาใช้ในการรักษา Premenstrual syndrome โดยทางเลือกในการรักษา จะเป็นการใช้แบบ Continuous oral contraceptive ปัจจุบัน 4th generation combined oral contraceptive pill (drospirenone) เช่น Yasmin มีฤทธิ์ที่ประกอบไปด้วย antimineralocorticoid antiandrogenic progestogenic effect เพิ่มขึ้น จึงถูกนำมาใช้ในการรักษา Premenstrual syndrome จากการศึกษาพบว่า การใช้ continuous oral contraceptive (90 mcg levonorgestrel/ 20 mcg ethinyl estradiol) ส่งผลทำให้อาการทางร่างกายและอาการซึมเศร้าดีขึ้น ประมาณ 30-59 เปอร์เซ็นต์ นอกจากนั้นการศึกษา Cochrane review 2012 1 หลังจากใช้ OCP (3 mg Drospirenone / 20 mcg EE ) 3 เดือน พบว่า ผู้หญิงที่มี PMDD อาการดีขึ้น แตในกลุ่ม PMS ยังมีหลักฐานที่ไม่เพียงพอ
2.3 Progesterone จากการศึกษาพบว่าประสิทธิภาพในการรักษา Premenstrual syndrome ยังไม่ชัดเจน
2.4 GnRH agonists มีผลในการยับยั้งการสร้าง ovarian steroid จึงมีประสิทธิภาพในการลดอาการทางกายมากกว่าพฤติกรรม อารมณ์และจิตใจ แต่เนื่องจากการใช้ GnRH agonist ในระยะยาว ส่งผลต่อการเกิดกระดูกพรุน (Osteoporosis) และเพิ่มความเสี่ยงต่อการเกิดโรคหลอดเลือดหัวใจ GnRH agonists จึงไม่นิยมเป็นทางเลือกแรกในการรักษา Premenstrual syndrome
2.5 Spironolactone เป็นยาในกลุ่ม Potassium-sparing diuretic ซึ่งมีฤทธิ์ Diuresis และ antiandrogenic effects ช่วยลดอาการปวดเต้านม (Breast tenderness) ท้องอืด (Bloating) น้ำหนักตัวเพิ่ม (Weight gain) และอารมณ์ซึมเศร้า (Depressed mood)
3. การรักษาแบบการผ่าตัด (Surgical treatment)
การผ่าตัดรังไข่ทั้งสองข้าง (Bilateral oophorectomy) เป็นการรักษาเพื่อยับยั้งการตกไข่อย่างถาวร ทำให้ Ovarian cycle ยุติลง ซึ่งข้อบ่งชี้ในการรักษาด้วยวิธีการผ่าตัด ได้แก่
- ผู้ป่วยที่ได้รับการวินิจฉัยว่าเป็น อาการก่อนมีประจำเดือนชนิดรุนแรง (Severe Premenstrual dysphoric disorder)
- ผู้ป่วยที่ไม่ตอบสนองต่อการรักษาด้วยยา (Failed medical therapy)
- ไม่สามารถใช้ยา GnRH agonist ในระยะยาวได้ (Unwilling to long term used of GnRH agonist)
- มีบุตรเพียงพอแล้ว (Complete childbearing)
| Drugs | Dose | Adverse effects | Symptoms targeted |
| Nutritional and herbal supplements | |||
| Calcium | 1200 mg/d | Constipation
Nausea Renal stone (dose>2500 mg/d) |
Mood symptoms, breast tenderness, bloating/swelling pain, headache, food craving |
| Vitamin B6 | 50-100 mg/d | Neurotoxicity
(dose >200 mg/d) Neuropathy |
Psychological |
| Chasteberry | Extract : 20/40 mg/d
Capsules : 200-400 mg/d |
Nausea/vomiting
Headache Bloating |
Breast tenderness, headache, irritability, anger, mood swings |
| Vitamin E | 150-400 IU/d | No significant adverse effects | Psychological and physical mastalgia |
| Other | |||
| Acupuncture | None | Physical symptoms | |
| Antidepressants (can be given continuously throughout cycle or just during luteal phase | |||
| Citalopram | 10-30 mg/d | Anxiety
Nausea Sleep disturbance Headache Sexual dysfunction |
Psychological |
| Escitalopram | 10-20 mg/d | Psychological | |
| Fluoxetine | 10-20 mg/d | Psychological and physical | |
| Paroxetine CR | 12.5-25 mg/d | ||
| Sertraline | 50-150 mg/d | ||
| Venlafaxine | 50-200 mg/d | ||
| Hormonal | |||
| Continuous oral contraceptive | 3 mg drospirenone/20 mcg ethinyl estradiol daily | Intermenstrual bleeding
Nausea Breast pain |
Psychological |
| 90 mcg levonorgestrel
/20mcg ethinyl estradiol daily |
Psychological and physical | ||
| Progesterone | 200-300 mg/d oral
300 mg/d vaginal |
Drowsiness | Psychological and physical |
ตารางที่ 3 แสดงการรักษา (Treatment) 7
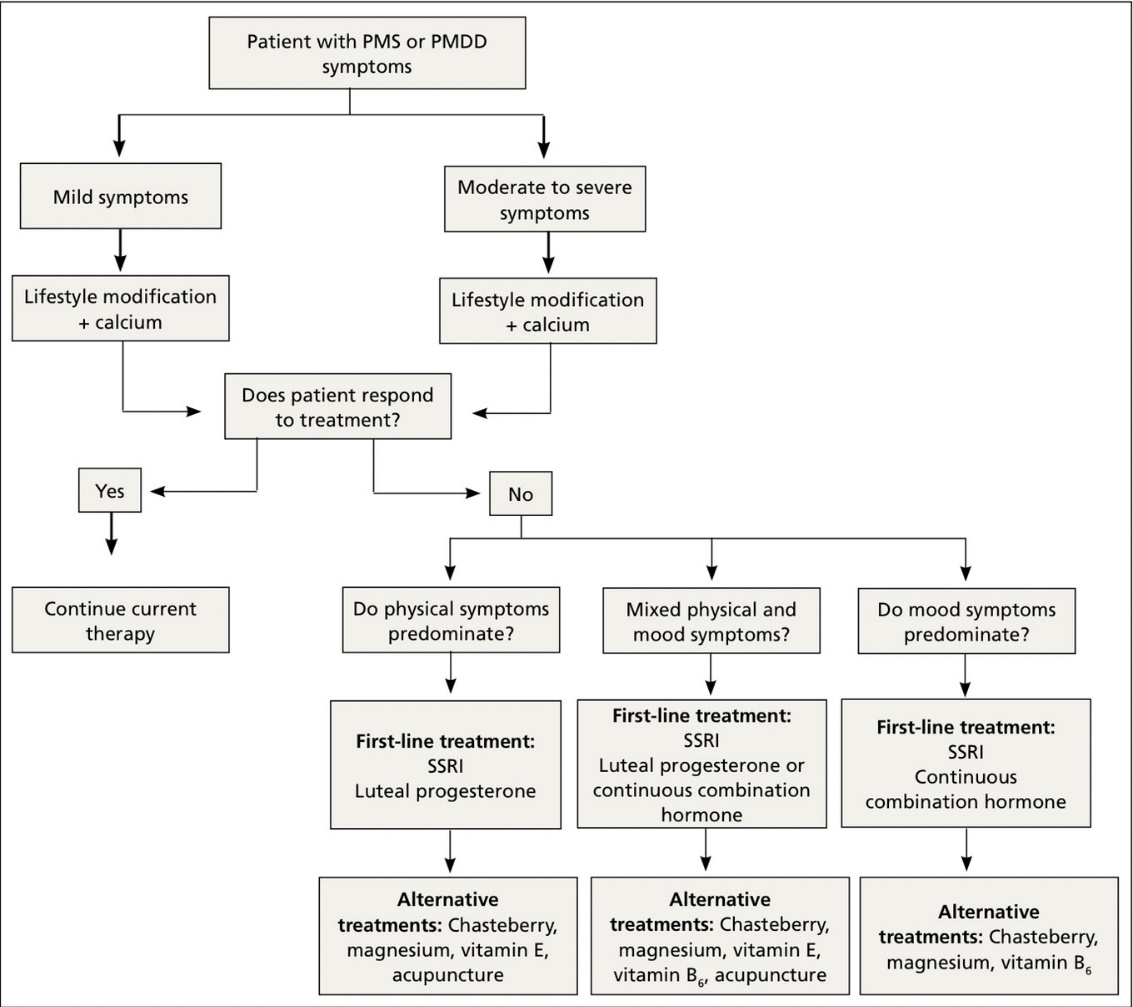
แผนภูมิที่ 1 แสดงแนวทางการรักษา (Treatment) 4
บทสรุป (Summary)
กลุ่มอาการก่อนมีประจำเดือน (Premenstrual syndrome) เป็นกลุ่มอาการที่ส่งผลต่อร่างกาย พฤติกรรม อารมณ์และจิตใจ ที่เกิดขึ้นในช่วงก่อนมีประจำเดือนของรอบเดือนนั้น และอาการจะหายไปได้เองในช่วงที่มีประจำเดือน ซึ่งอาการเหล่านั้นส่งผลต่อการใช้ชีวิตประจำวัน โดยเป้าหมายหลักของการรักษาก็คือการลดอาการที่ผู้ป่วยประสบอยู่ทั้งด้านร่างกายและจิตใจ ซึ่งการรักษามีทางเลือกหลากหลายวิธี ทั้งการใช้ยาในการักษา และการไม่ใช้ยาในการรักษา และหากการใช้ยาไม่สำเร็จผล จึงจำเป็นที่ต้องใช้การรักษาด้วยวิธีการผ่าตัดเข้ามาช่วยในการรักษาต่อไป การดูแลรักษาผู้ป่วยในกลุ่มนี้จึงต้องอาศัยความร่วมมือทั้งจากผู้ป่วย แพทย์เฉพาะทางด้านนรีเวชกรรมและด้านจิตวิทยา เพื่อให้การรักษาเหมาะสมกับผู้ป่วยมากที่สุด นอกจากนี้ยังต้องมีการศึกษาเพิ่มเติม เนื่องจากการศึกษาเกี่ยวกับภาวะนี้ ยังมีข้อมูลน้อยและมักเป็นการศึกษาขนาดเล็กประกอบกับตัวชี้วัดด้านอาการของผู้ป่วยยังมีความหลากหลาย
เอกสารอ้างอิง
- Hofmeister S, Bodden S. Premenstrual Syndrome and Premenstrual Dysphoric Disorder. Am Fam Physician. 2016;94(3):236-40.
- Biggs WS, Demuth RH. Premenstrual syndrome and premenstrual dysphoric disorder. Am Fam Physician. 2011;84(8):918-24.
- Berek JS, Berek DL. Chapter 23 Common psychiatric problems, Premenstrual syndrome and premenstrual dysphoric disorder. Berek & Novak’s Gynecology 16th edition. NewYork. Wolters Kluwer2020. 509-10 p.
- Yonkers KA, Casper RF. Epidemiology and pathogenesis of premenstrual syndrome and premenstrual dysphoric disorder UpToDate. Waltham, MA: UpToDate Inc. [Available from: https://www.uptodate.com. (Accessed on November 20, 2022.)
- Yonkers KA, CAsper RF. Clinical manifestations and diagnosis of premenstrual syndrome and premenstrual dysphoric disorder UpToDate. Waltham, MA: UpToDate Inc. [Available from: https://www.uptodate.com. (Accessed on November 20, 2022.)
- Casper RF, Yonkers KA. Treatment of premenstrual syndrome and premenstrual dysphoric disorder UpToDate. Waltham, MA: UpToDate Inc. [Available from: https://www.uptodate.com. (Accessed on November 20, 2022.)
- Danis P, Drew A, Lingow S, Kurz S. Evidence-based tools for premenstrual disorders. J Fam Pract. 2020;69(1):E9-e17.
- Kwan I, Onwude JL. Premenstrual syndrome. BMJ Clin Evid. 2015;2015.
- Dilbaz B, Aksan A. Premenstrual syndrome, a common but underrated entity: review of the clinical literature. J Turk Ger Gynecol Assoc. 2021;22(2):139-48.
- Ryu A, Kim TH. Premenstrual syndrome: A mini review. Maturitas. 2015;82(4):436-40.
- Ismaili E, Walsh S, O’Brien PMS, Bäckström T, Brown C, Dennerstein L, et al. Fourth consensus of the International Society for Premenstrual Disorders (ISPMD): auditable standards for diagnosis and management of premenstrual disorder. Arch Womens Ment Health. 2016;19(6):953-8.