By Asst. Prof. Dr. Nawat Watanachai
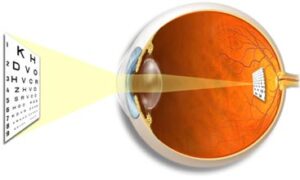
Our eyes are as simple as a camera. What do we look at? Light passes through the cornea and lens, both of which It's like a camera lens system. The refracted image of the cornea and the lens of the eye falls on the retina, which acts like a camera film, between the lens of the eye. and retina There will be a portion of clear water. Jelly-like appearance, called vitreous or vitreous.
When we are young, the vitreous is clear, free of sediment, and attaches to the front of the retina. Attached to the back of the lens when there is something like
– Age over 40 (signs of aging begin to come….hehe)
– Had an accident that hit the eye or have had eye surgery before
– Nearsightedness, especially shorter than 600
– Have had severe eye inflammation (uveitis)
– Some diseases of the vitreous eye, such as Jansen disease, Wagner disease, Stickler syndrome, have only strange names.
Which deterioration will have two major stages
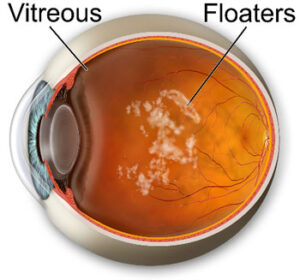
1. Vitreous becomes cloudy as sediment (vitreous syneresis, vitreous degeneration, vitreous liquefaction) – In fact, eye-popping It's not a clear, basic jelly like Pipo or jelly, but it's actually a network of collagen fibers. which contains up to 90% water, these collagen fiber networks Normally, it's a fine line. orderly making us unable to see the shadows of these fibers
deteriorated eyes these collagen fibers Some lines will be torn into pieces. Some fibers are thicker. clump together and lose clarity make people who have cloudy eyes start to see sediment This may be described as spider webs, dots, lines or mists floating around as you roll your eyes. (Because when we roll our eyes Vitreous will drift away as well) most often do not see these sediments all the time. Can be seen only when the conditions of the light are suitable, such as looking out at the sky on a bright day, reading a book roll eyes left and right Causing eyes to move back and forth a lot see it easier, etc.
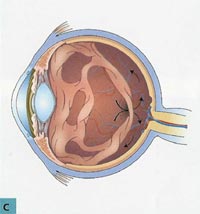
2. Vitreous detachment from the retina (posterior vitreous detachment) – Thao a little more. that our eyes will attach to each part of the retina with unequal strength the point where it clings the tightest located in front of the retina near the back of the lens We call this area the base of the vitreous (I don't know how to translate it from the word vitreous base). around the edge of the optic disc, the macula, and along the retinal vessels
Therefore, when the vitreous shrinks It therefore tends to gradually separate from the posterior retina. near the optic nerve with the receiving point first and move towards its base in front of it at this distance Some patients may notice sediment increasing rapidly, because often the vitreous at the edge of the optic nerve terminal. will thicken in a circular line When the eyes suddenly separated This ring will make the patient see the shadow as a crooked ring of it right away. (which when the vitreous comes out of the optic nerve terminal This band will be crooked or yo-yo) Many patients will tell clearly that seen as a curved shadow Or in a circle, oval, floating around the corner of the eye – floaters
Sometimes, some people, when they roll their eyes quickly in the dark The vitreous will swing to hit the retina. or tension on the retina at the junction between the vitreous part of the eye that has separated from the retina with the vitreous part still attached to the retina This mechanically stimulates the retina. And it will be misinterpreted as flashing light – flashing – probably similar to how some of you 'see stars' when they get punched. with the retina Our eyes will create clear water to fill it.
After many months when separation is complete Flashing light will be less. and gradually disappeared
The vitreous sediment gradually persists for months or even years. Make the person see these dots and lines for a while. then gradually decrease (where the person was noticing its shadow falling Because the vitreous shrinks more These sediments will float to the front. more and more distant from the retina makes the patient notice less of its shadow can see shadows more easily and clearly than objects far from the scene)
In general, this is the only story. Which we don't have to do anything because most of them are just annoying.
Except that
1. Some lumps of sediment in the vitreous are so large that a lunar phenomenon occurs…this is too big…to the point of obscuring vision. may use a laser to break these large sediment down - this method is not standard. considered an experiment because there is a high risk if bad luck The laser does not hit the sediment. go to the retina at the point of receiving the image instead, it can be messy, possibly to the point of being stuck together for life
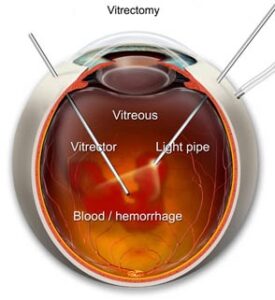
2. There is a lot of sediment. Until the vitreous is completely cloudy, making it blurry. This can be surgically washed to remove the sediment (pars plana vitrectomy).

But there will be some people who have other issues. which is serious
1. Bleeding in the vitreous (vitreous hemorrhage) as mentioned above. Vitreous sticking to the retina is quite strong along the blood vessels. Sometimes, if there is some point where it sticks very tightly when the vitreous shrinks Vitreous eyes may not be separated. Instead, it causes the walls of blood vessels to tear. The blood then poured into the vitreous and the space between the vitreous and the retina. Immediately makes the patient very dim. (looks like fog)
if in low light The patient will see it as a shadow.
If in bright light, in the sun or using a flashlight to shine Some people can see it as bright red blood.
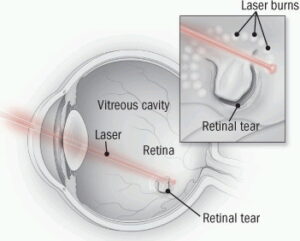
2. Retina tear (retinal break, retinal tear) The reason is the same as No. 1, during the vitreous contraction. Some points where the vitreous cling to the screen is tighter than usual. will pull the screen to tear
If the image screen is torn (There may be bleeding like No. 1, with or without it.) The patient will see flashes of light very often. because when you roll your eyes The torn area of the retina moves more than usual. (Because there are still vitreous eyes that easily slide and cling) Some people say they see these flashes. One day five sixty times
In this case, if nothing is done, there are two possibilities.
– The vitreous eye separates from the torn part of the retina by itself, this is the end, you don't have to do anything.
– Villous eyes pulling the retina more and more. until the entire retina peels off (go to item 3)
3. Retinal detachment. This item is the worst. The retina detaches from the inner eyeball. (Imagine trying to get a spoon to scrape the burnt coconut flesh out of the coconut into one big chunk. gives me the same feeling)
Our retina a thin tissue But it also consists of 10 thinner layers.
-
- The inner sublayer, close to the vitreous, relies on the blood supply from the retinal blood vessels itself.
-
- The outer subfloor Relies on blood from the blood vessels of the choroid layer, which is beyond the retina.
-
- So if it comes off, the outer sublayer lacks blood supply – our photoreceptors, rods and cones, are in this outermost sublayer. It will gradually die.
- Repair can be done by reattaching the dislocated retina, which is cumbersome, tortures the patient and in some cases causes exhaustion for both doctors, patients and relatives.
| The general procedure that we do when a patient comes in with sediment/fog/floating matter is that we tend to dilate the iris. Check to see if there is macular degeneration/retinal tear/retinal detachment.
1. If there is a retinal detachment, it will be sent to a retinal specialist (retina specialist) for surgery. 2. If there is a tear in the retina, it can be laser or chilled. and then check again – Come to see me by appointment. |