
Physical Examination
GA: Alert, no dyspnea
VS: HR 152/min, RR 44/ min, BP 81/ 42 mmHg, O2 sat 98%
BW 4.2 KG (25th percentile), Ht 54 cm (< 3th percentile)
HEENT: no hoarseness
Chest: Lung- no adventitious sound
Heart: PSM grade 3/6 at LLSB, increased P2 intensity
Abdomen: no hepato-spenomegaly
Extremity: no edema
CNS: normal deep tendon reflex
Other: unremarkable
Laboratory Investigations
BUN = 3 mg/dl, Creatinine = 4 mg/dl, Na =136 mEq/L, K= 5.1, Cl =102, CO2CP =19
CBC: Hb=9.6 mg%, Hct = 27.2 vol%, WBC 6,900 mm3 ( N= 10.2, E= 2.8, B = 1.2, L= 69.8, M = 16) Platelet = 285,000 mm3, MCV 82
Fig1. CXR shows global cardiomegaly (without increased pulmonary blood flow)

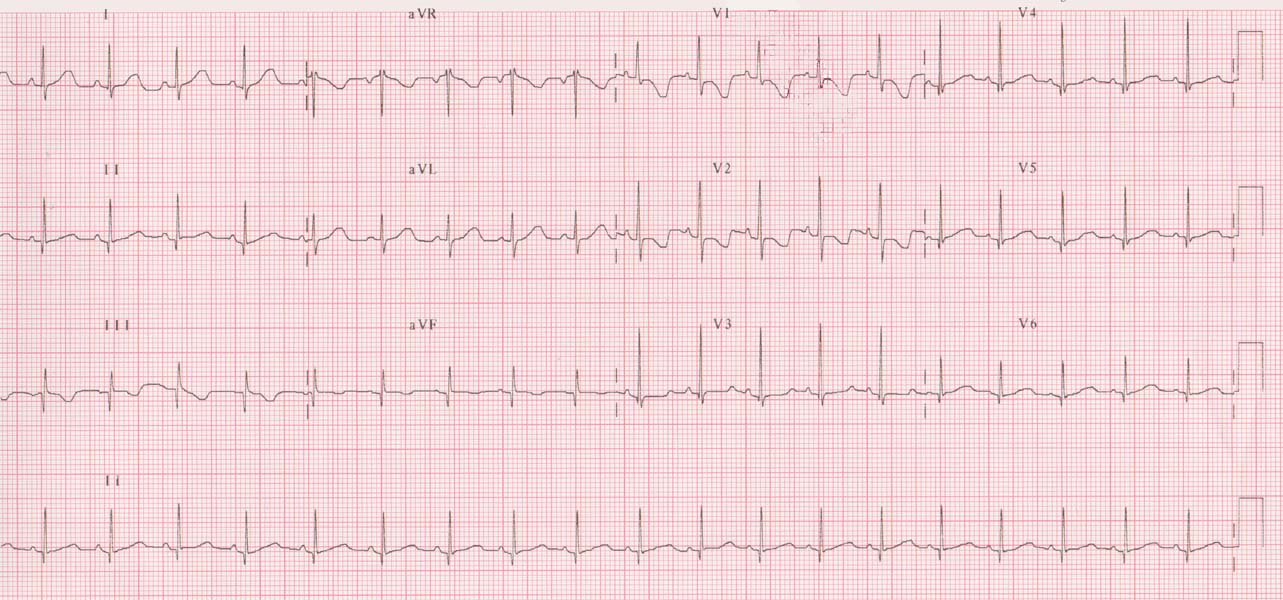
Fig 2 EKG พบมี RVH จาก upright T in V1 และ inverted T wave in lead I, aVL,V5,6
Echocardiogram:
Markedly dilated RA and RV, flattening of IVS .
Patent foramen ovale 1 mm with right to left shunting.
Moderate TR, Peak TR gradient 95 mmHg. Mild PR with PR gradient 15 mmHg.
Good LV and RV systolic function.
Echo diagnosis: Severe pulmonary hypertension
Clinical diagnosis: Cardiac beriberi
Therapeutic diagnosis: Thiamine 50 mg IV 3 วัน (และให้ thiamine 50 mg oral ต่ออีก 2 สัปดาห์)
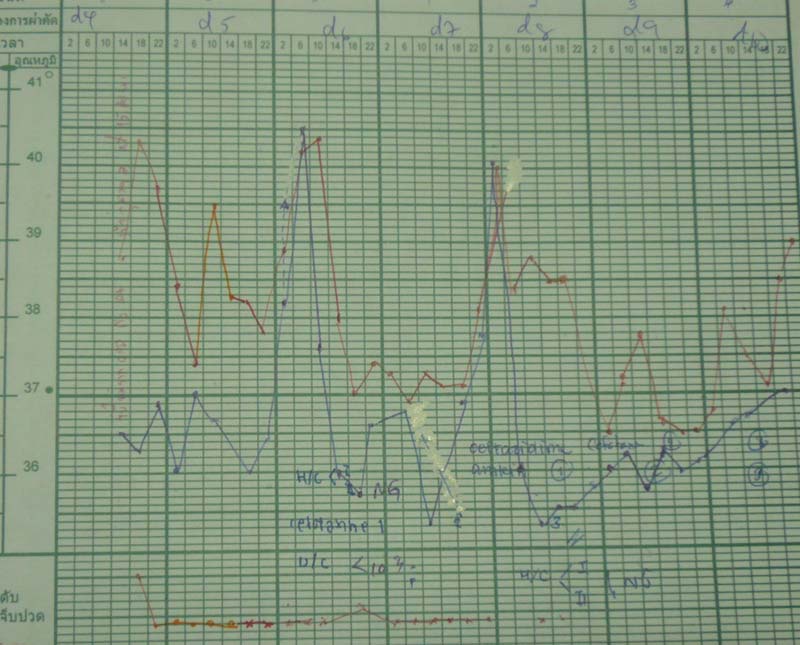
หลังให้ thiamine เข้าทางหลอดเลือดดำในวันแรกผู้ป่วยมี diuresis มากกว่า 2 ซีซีต่อชั่วโมง แต่ไม่มีหัวใจเต้นช้าลง, BP เพิ่มเป็น 100/42 mmHg ใน วันที่ 2
วันที่สี่หลังไดรับ thiamine ตรวจ echocardiogram พบ RA และ RV ลดขนาดลงเกือบปกติ mild TR, TR gradient ลดเหลือ 35 mmHg
Fig 3 EKG 5 วันหลังการรักษาด้วย thiamine พบ T wave กลับมาเป็นปกติ และ T wave กลับมาหัวตั้งใน lead I, aVL,V5,6
Discussion:
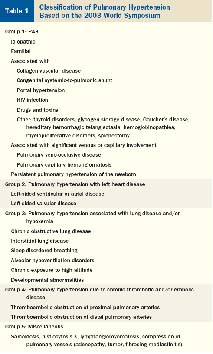 Infant ที่มาด้วย pulmonary hypertension ที่อายุต่ำกว่า 1 ปี สาเหตุส่วนใหญ่จะมาจาก congenital heart disease หรือ lung disease1 และถ้าหากพบในทารกแรกเกิดมักจะเป็น persistent pulmonary hypertension of the newborn ในตารางที่ 12 สาเหตุอื่นๆหรือ idiopathic PAH อาจพบไม่บ่อยใน age group นี้
Infant ที่มาด้วย pulmonary hypertension ที่อายุต่ำกว่า 1 ปี สาเหตุส่วนใหญ่จะมาจาก congenital heart disease หรือ lung disease1 และถ้าหากพบในทารกแรกเกิดมักจะเป็น persistent pulmonary hypertension of the newborn ในตารางที่ 12 สาเหตุอื่นๆหรือ idiopathic PAH อาจพบไม่บ่อยใน age group นี้
ผู้ป่วยรายนี้อายุ 2 เดือน อาการและ CXR ไม่เข้ากับโรคปอด การตรวจ echocardiogram ไม่พบโรคหัวใจที่เป็นสาเหตุ ประวัติ ตรวจ ร่างกายไม่เข้ากับ HIV, collagen vascular diseases, portal hypertension, thyroid disease, etc. แต่ มีประวัติทานนมแม่ซึ่งแม่อยู่ในชนบทที่อาจจะได้ thiamine จากอาหารไม่เพียงพอ3 จึงน่าจะนึกถึง cardiac beriberi มากที่สุด และ
เนื่องจากเป็นโรคที่ตอบสนองต่อการรักษาเร็ว ค่ายาไม่แพง
จึงควรให้การรักษาโดยให้ thiamine ไปก่อนแม้ไม่ได้ผลการตรวจทางห้องปฏิบัติการณ์ที่แน่นอน (เช่น TPP,ETK หรือ thiamime level)
ในผู้ป่วยรายนี้ผู้ป่วยตอบสนองดีต่อ thiamine โดย มี diuresis ขนาดหัวใจเล็กลง และความดันในปอด
ลดลงอย่างรวดเร็วจึงช่วยสนับสนุนการวินิจฉัยโรคขาด thiamine หรือ cardiac beriberi
Cardiac beriberi เป็นโรคพบไม่บ่อย ในผู้ใหญ่พบในพวก alcoholic ในเด็กพบในพวกขาด thiamine ในอาหาร ซึ่งพบได้ในแถบเอเชีย ทั้งในฟิลิปปินส์ มาเลเซีย อินโดนิเชียและไทยซึ่งมีข้าวที่สีเป็นอาหารหลักของประชากร อย่างไรก็ตามปัจจุบันในประเทศเหล่านี้พบน้อยลงเนื่องจากมีการปรับปรุงการรับประทานอาหารให้ดีขึ้น3 ยกเว้นในประเทศไทย4 และลาว5 ยังพบรายงานในบริเวณที่ประชากรมี low socioeconomic และ low education ซึ่งมี thiamine consumption ไม่พอเพียง เนื่องจากการรับประทานชนิดของอาหารไม่ได้สัดส่วน ส่วนในประเทศที่พัฒนาแล้วพบน้อยมากในเด็ก มีเพียงรายงานในอิสราเอลในเด็ก infants 9 รายที่ได้รับนมผสมจากถั่วเหลืองที่ใส่ thiamineน้อยมาก จึงเกิดอาการขาด thiamine รุนแรง6 ในเด็กเล็กมักจะเป็น infantile beriberi และมาด้วยเรื่องหัวใจล้มเหลวร่วมกับความดันในปอดสูง. Thiamine มีอยู่ในอาหารจำพวกเนื้อสัตว์ ปลา ถั่วเขียว เมล็ดพืช (cereal, grains) อาหารบางอย่างจะไปทำลาย thiamine เช่นปลาร้า ชา ใบเมี่ยง และภาวะบางอย่างร่างกายต้องการใช้ thiamine มากขึ้นเช่น ติดเชื้อ ตั้งท้อง ให้นมบุตร ขนาด thiamine ที่ควรรับประทานในเด็ก infant (RDA) คือ 0.5 มก.ต่อวัน มารดาที่ให้นมลูกควรได้ขนาด 1.4 มก.ต่อวันเป็นอย่างน้อย
Pathogenesis: Thiamine เป็น ส่วนประกอบของ coenzyme thiamine pyrophosphate (TPP) ที่สำคัญใน carbohydrate metabolism (Kreb cycle) เพื่อให้ได้เป็น พลังงาน (ATP) การขาด thiamine มีผลต่อ carbohydrate metabolism ที่หัวใจ ทำให้กล้ามเนื้อหัวใจขาดพลังงานและทำงานผิดปกติ ส่วนที่เส้นเลือดพบว่าการขาด thiamine ทำให้มี massive capillary dilatation ในกล้ามเนื้อลายอย่างมากซึ่งมีผลคล้ายกับ A-V anastomosis จึงเกิดเป็น high output cardiac failure ตามมา ในเด็กเล็กหากเป็นนานขึ้นจะเปลี่ยนเป็น low cardiac output failure หรือที่เรียก “Shoshin beriberi” หรือ acute fulminant form ทำให้เสียชีวิตได้หากรักษาไม่ทัน
Histopathology: กล้ามเนื้อหัวใจมีลักษณะของ interstitial fibrosis, variation in size of myocardoial fibers, mild myocyte hypertrophy และ disarrangement of myocytes.7
Hemodynamics: มีการศึกษาhemodynamics โดย cardiac catheterization เฉพาะในผู้ใหญ่หรือเด็กโตเท่านั้น เพราะเด็กเล็กมักจะมีอาการหนักและได้รับการรักษาไปก่อน ผลการศึกษาพบว่ามี cardiac output สูง ความดันใน RA, RVED สูงขึ้น และ PA pressure มักจะสูง ซึ่งความดันที่สูงขึ้นเหล่านี้น่าจะเป็นผลจาก cardiac output ที่เพิ่มขึ้น8 ดังเช่นที่พบใน hyperthyroidism ส่วน systemic vascular resistance จะต่ำซึ่งเป็นผลจากการขาดB1โดยตรง9
Clinical manifestations: Cardiac beriberiในเด็กพบอุบัติการณ์สูงในสองระยะคือเด็กเล็กและเด็กโต ในเด็กเล็กมักพบในอายุต่ำกว่า 2 ปี และพบบ่อยในช่วง2-3 เดือน (infantile beriberi) มีประวัติรับประทานแต่นมมารดา โดยทั่วไปน้ำนมคนมีระดับ thiamine 20 ไมโครกรัม/มล. เมื่อเปรียบเทียบกับนมวัวซึ่งมี 40ไมโครกรัม/มล. มารดาอาจมีประวัติชาปลายมือปลายเท้าจากขาด thiamine ทารกอาจมี subclinical ของ thiamine deficiency อยู่ก่อน แล้ว precipitate โดย infection หรือ stress ซึ่งทำให้ต้องการ thiamine มากขึ้น ผู้ป่วยอาจมาด้วยอาการ irritable, anorexia, hoarseness และอาการของ biventricular failure ที่ซีกขวาเด่นคือ tachycardia, dyspnea, enlarged liver & spleen, generalized edema และ ascites ตรวจที่หัวใจมักไม่พบ significant murmur, หากฟังได้ murmur จะเป็น tricuspid regurgitation จาก pulmonary hypertension อาจฟังได้ S3 gallop และเสียง pulmonic second heart sound ดังขึ้นและคลำได้ RV heaving (จากpulmonary hypertension) อาจมี signs ของ low output stage คือ anuria (decreased renal blood flow) ถ้าอาการรุนแรง (“Shoshin beriberi”) จะมี pallor or peripheral cyanosis, cool extremities and weak pulse และมี severe metabolic acidosis จาก lactic acidosis ผู้ป่วยอาจเสียชีวิตใน 36-48 ชั่งโมงถ้าไม่ได้รับ thiamine รักษา อาการทางระบบประสาทที่พบร่วมอาจมี decreased deep tendon reflex, convulsion และ unconscious ได้ ในเด็กโตพบcardiac beriberi น้อยมาก มักมาด้วย high output failure, bounding pulse, tachycardia, อาจมีอาการปวดน่อง ชาทั่วไป หรือชาตามปลายมือปลายเท้าเช่นเดียวกับในผู้ใหญ่ได้
จากการรวบรวมผู้ป่วย cardiac beriberi ที่มารักษาที่ภาควิชากุมารเวชศาสตร์ มหาวิทยาลัยเชียงใหม่ ระหว่างปีพ.ศ.2542-2546 จำนวน 9 ราย เป็นหญิง 6 ราย (67%) อายุเฉลี่ย 3 เดือน (2-6 เดือน) พบภาพรังสีทรวงอกมี cardiomegaly with pulmonary venous congestion ทุกราย หัวใจมีรูปร่างเป็น globular shape หรือ RV dilatationบางราย คลื่นไฟฟ้าหัวใจมี right axis deviation และ ลักษณะของ RVH abnormal for age ทุกรายและส่วนใหญ่จะมี strain pattern ร่วมด้วย Echocardiogram ก่อนให้ thiamine พบว่าทุกรายมี RA และ RV dilatation ร่วมกับ pulmonary hypertension, mean TR gradient 53 mmHg (range 30-90 mmHg), normal LV fractional shortening และ ejection fraction บางรายอาจพบpericardial effusion ร่วมด้วยแต่มีปริมาณเพียงเล็กน้อยเท่านั้น
การวินิจฉัย : ใช้อาการทางคลินิก ภาพรังสีทรวงอกพบหัวใจโตทั่วไป มี pulmonary venous congestion และคลื่นไฟฟ้าหัวใจในเด็กเล็กพบ sinus tachycardia, RAD, RVH อาจมี strain ร่วมด้วย เด็กโตอาจพบเพียง low QRS voltage และ ST-T wave changes. ในโรงพยาบาลที่ไม่มีการตรวจยืนยันทางห้องปฏิบัติการ อาจใช้ therapeutic diagnosis ด้วยการให้ thiamine 25-50 มก.(เด็กเล็ก) หรือ 50-100 มก.(เด็กโต) ทางหลอดเลือดดำหรือเข้ากล้าม 3-5 วัน แล้วดูการตอบสนองคือ diuresis ภายใน 1-2 ชั่งโมง, transient decreased heart rate และ increased blood pressure ภายใน 12 ชั่งโมง, และ CHF symptoms ดีขึ้นใน 24 ชั่วโมง ส่วนขนาดของหัวใจจากภาพรังสีทรวงอกกลับมาปกติใช้เวลาเป็นสัปดาห์ การวัดความดันในปอดโดย echocardiogram พบว่า TR gradient ลดลงอย่างรวดเร็วภายใน 1-2 วันหลังให้ thiamine
การตรวจทางห้องปฏิบัติการ: ที่นิยมในอดีตคือ erythrocyte transketolase (ETK) activity จะลดลง, หรือ thiamine pyrophosphate (TPP effect) พบว่ามากกว่า 15% หรือ ตรวจ urine thiamine level ที่ลดลง ปัจจุบันการตรวจ thiamine diphosphate(TDP) level ในเม็ดเลือดแดงด้วยวิธี HPLC 10 เป็นวิธีที่วัดระดับ thiamine ที่สะสมไว้ในร่างกายโดยตรง การเก็บตัวอย่างคงตัวดีกว่า ผู้ป่วยที่มีปัญหาโรคตับหรือโรคไตจะไม่มีผลต่อการตรวจวิธีนี้ดังเช่นในสองวิธีแรก
การรักษา: ควรให้ thiamine ต่อไปจนถึง 2 สัปดาห์หากอาการรุนแรง บางรายอาจจำเป็นต้องได้รับยาขับปัสสาวะหรือ inotropic drug ร่วมด้วย หลังจากนั้นควรให้ maintenance ด้วย B 1-6-12 รับประทานต่อประมาณ 1-2 เดือน การรักษาต้องรักษามารดาไปด้วยและให้คำแนะนำมารดาเกี่ยวกับการรับประทานอาหารที่มีสารอาหารครบถ้วนเป็นสิ่งจำเป็นเพื่อไม่ให้เกิดโรคซ้ำอีก
สรุป ภาวะ pulmonary hypertension ใน cardiac beriberi เป็น reversible process จาก high cardiac output เมื่อรักษาที่สาเหตุแล้วจะทำให้ภาวะนี้หายไปอย่างรวดเร็วจึงไม่จำเป็นต้องใช้ pulmonary vasodilator ในผู้ป่วยกลุ่มนี้ แต่ในแง่ของการวินิจฉัยควรจะอยู่ในการวินิจฉัยแยกโรคของผู้ป่วยที่มาด้วยความดันในปอดสูงโดยเฉพาะในเด็กทารก
References:
1 Hoehn T. Therapy of pulmonary hypertension in neonates and infants. Pharmacology & Therapeutics 2007;114: 318–26.
2 Chin KM, Rubin LJ. Pulmonary arterial hypertension. J Am Coll Cardiol 2008; 51:1527–38.
3 Phornphutkul C, Yingkamol M, Thanangkul O. Cardiac beriberi in infants and children. An analysis of seventy-five cases. In Ped. Cardiology Vol 4. Godman MJ. ed. Edinburgh, Churchill Livingstone.1981:712-20.
4 McGready R, Simpson JA, Cho T, et al. Postpartum thiamine deficiency in a Karen displaced population. Am J Clin Nutr. 2001;74:808-13.
5 Soukaloun D, Kounnavong S, Pengdy B, et al. Dietary and socio-economic factors associated with beriberi in breastfed Lao infants. Ann Trop Paediatr. 2003;23:181-6.
6 Fattal-Valevski A, Kesler A, Sela B, et al. Outbreak of life-threatening thiamine deficiency in infants in Israel caused by a defective soy-based formula. Pediatrics 2005;115;e233-e238
7 Kawano H, Hayashi T, Koide Y, et al. Histopathological changes of biopsied myocardium in Shoshin beriberi. Int Heart J 2005;46:751–9.
8 Park JH, Lee J, Jeong J, et al. Thiamine deficiency as a rare cause of reversible severe pulmonary hypertension. International Journal of Cardiology 2007;121: e1–3.
9 Akbarian M, Yankopoulos N, Abelmann W. Hemodynamic studies in beriberi heart disease. Am J Med 1966;41:197-211.
10 Talwar D, Davidson H, Cooney J, St. JO’Reilly D. Vitamin B1 status assessed by direct
measurement of Thiamin Pyrophosphate in erythrocytes or whole blood by HPLC:Comparison with Erythrocyte Transketolase Activation Assay. Clinical Chemistry 2000;46: 704–10.
Ass. Prof. Yupada Pongprot

